 Portuguese
Portuguese  English
English  Spanish
Spanish 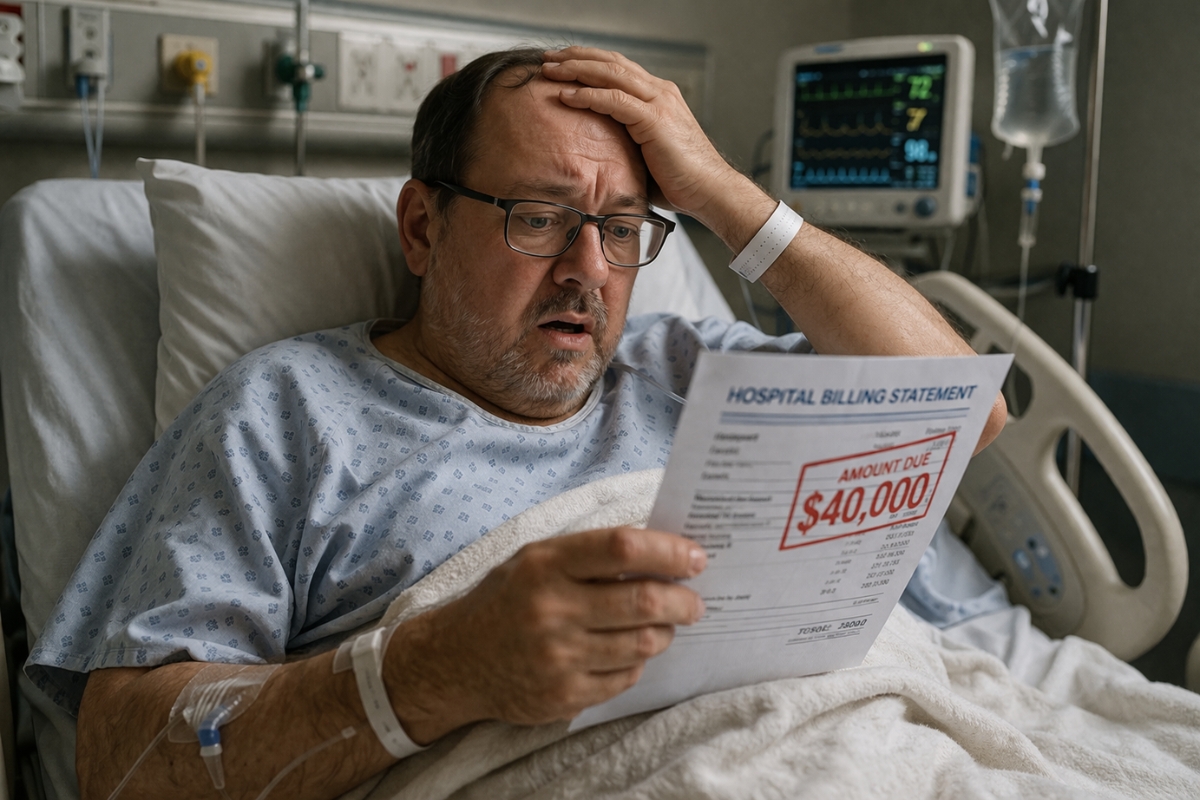
Ricardo Molina’s experience reveals how hospital care in the United States charges not only for the final diagnosis but for the entire machinery set in motion to rule out risks, creating exorbitant bills even when the patient is discharged with the news that everything is fine.
A sudden malaise, a sharp drop in blood pressure, emergency care, tests, observation, and a procedure to rule out cardiac risk. In the end, the medical news was a relief: the heart was fine. But the real shock came later, in the bill.
In a video posted on social media, Ricardo Molina shares an experience that summarizes the logic of the healthcare system in the United States: the patient can leave the hospital medically stable but financially shaken.
The case draws attention because it shows something that many people outside the U.S. do not immediately understand. In the American system, the cost of a hospital visit does not depend solely on the final diagnosis. It depends on the entire structure mobilized to investigate a possible risk. And this means that even when “it was nothing serious,” the bill can include ambulance, emergency room, medical team, tests, monitoring, short hospitalization, and additional procedures.
-
Silent heart disease raises alarm after bodybuilder’s death and exposes how genetics, anabolic steroids, and intense training can become a dangerous combination

-
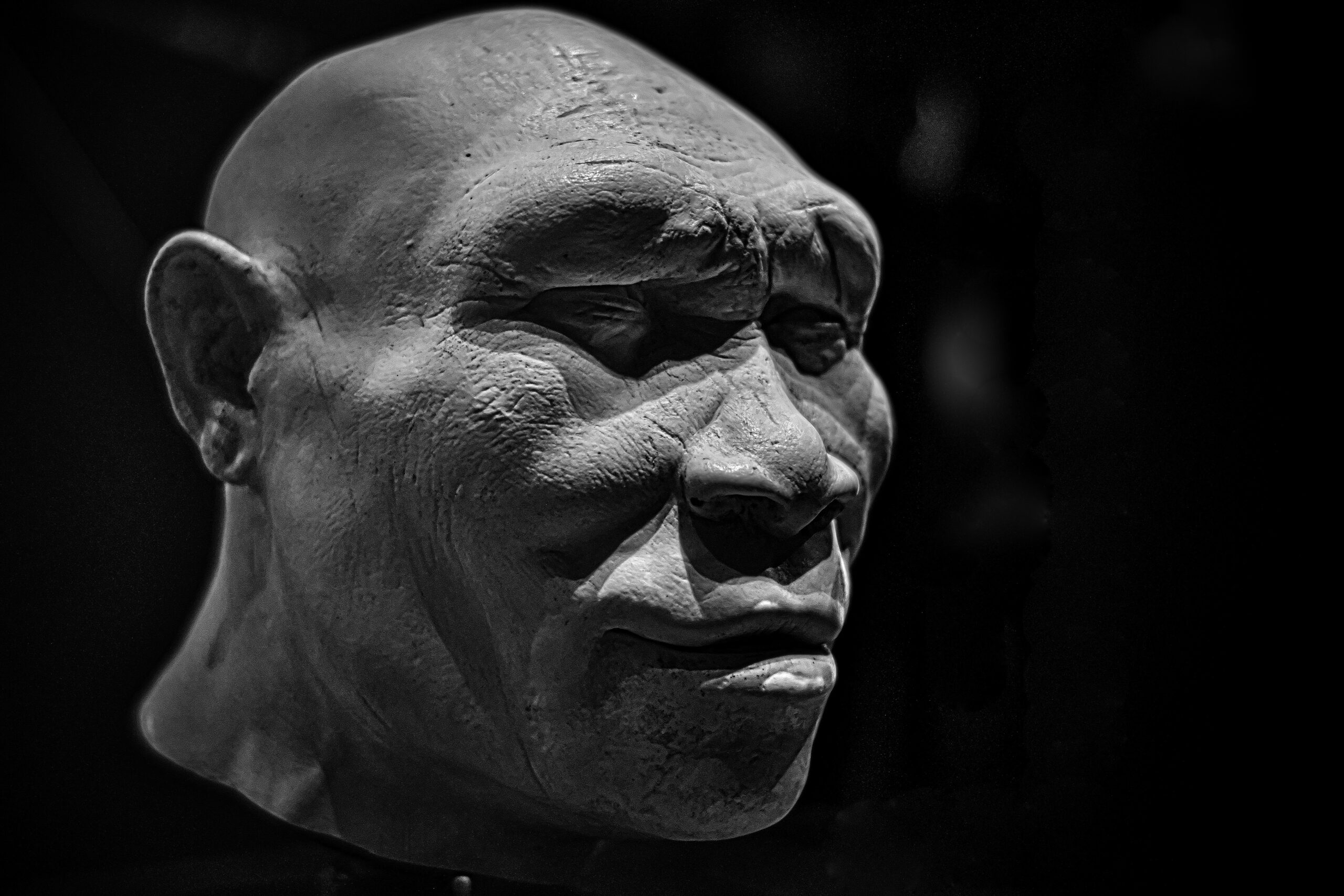
Six 400,000-year-old teeth found in China contained a protein that was believed to exist only in the mysterious Denisovans: the discovery reveals that Homo erectus interbred with this extinct relative and left a genetic trace that still lives in human populations today.

-
American donated US$ 5,000 to a Chinese farmer to plant trees in the desert, and decades later the money turned into a forest with more than 50,000 trees.
-
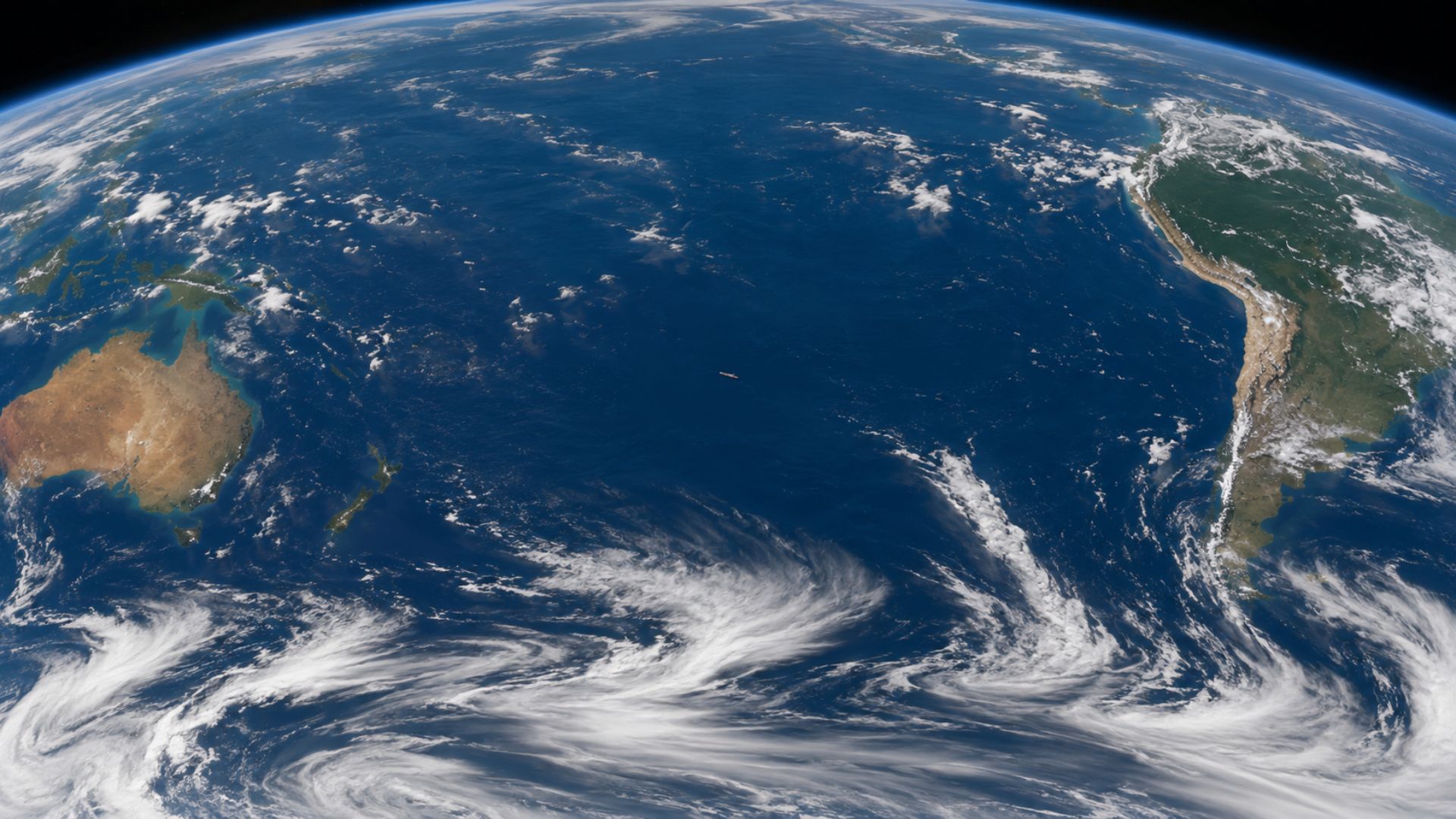
Almost no ship sails directly between South America and Australia, and the reason is a combination of the vast distance, winds that circle the planet nonstop, and the absence of ports along the way, leaving the South Pacific as a water desert.



The problem is not just the test. It is the entire machinery
When a patient enters the emergency room, the American emergency department, they become part of the most expensive entry point of the system. The hospital does not charge just for the consultation: it charges for the triage, for the emergency structure, for the team, for diagnostic resources, and often for doctors and services billed separately.
In situations of suspected cardiac issues, for example, it is common for the protocol to be aggressive in ruling out greater risks. This helps explain why a situation that started as malaise can end in hospital observation, imaging tests, monitoring, and even invasive procedures.
Even without confirming the exact value of the reported case, an estimate of tens of thousands of dollars for a night in the hospital with cardiac investigation does not sound absurd within the American reality. Public transparency data shows that cardiac diagnostic procedures can cost thousands of dollars on their own, not counting the emergency room, medical fees, and hospital stay.
In the U.S., choosing the wrong door can be costly
The big lesson from the episode is practical: in the United States, hospitals are for real emergencies.
This does not mean minimizing serious symptoms. If there are signs consistent with heart attack, stroke, severe respiratory distress, significant trauma, or another potentially fatal condition, the emergency room remains the right place. The insurers and health organizations themselves in the U.S. emphasize that the ER should be used in life-threatening situations or those with serious harm risk.
But outside of these scenarios, the financial logic of the system favors other entry points. For less serious problems, the smartest move is usually to seek urgent care, outpatient clinics, primary care, or telemedicine, which typically cost much less than a trip to the hospital.
The medical scare turns into financial scare
The story shared by Ricardo Molina touches on a sensitive point for those living, traveling, or planning to live in the United States: the fear is not just about feeling unwell. It is not knowing how much that care will cost later.
In many countries, the focus of emergency care is purely clinical. In the U.S., it is also economic. An episode that ends in relief from a medical standpoint can turn into months of negotiation, billing, insurance deductible, copayment, or debt.
The lesson that remains
The account goes viral because it conveys an uncomfortable truth: in the United States, getting sick or simply “feeling unwell” can be expensive even when nothing serious is confirmed.
Therefore, understanding when to go to the hospital and when to seek a clinic or urgent care is not just a matter of convenience. It is also a financial decision.
In the end, the experience exposes one of the harshest faces of the American system: sometimes, the diagnosis reassures — but the bill is what truly keeps one awake at night.






Be the first to react!